Cryptogenic ischemic strokes are symptomatic cerebral infarcts for which no probable cause is identified after adequate diagnostic evaluation. More expansive definitions add strokes in patients who are incompletely evaluated and in those with more than one probable cause identified, but these are better considered to be separate entities. Among strokes of undetermined cause, useful further distinctions are between those that are cryptogenic after standard evaluation and those that are cryptogenic after additional, specialized evaluation and between those that are “highly cryptogenic” (i.e., with no probable and no possible cause discovered) and those “of possibly determined origin” (i.e., with no probable, but one or more possible, causes identified).
Cryptogenic mechanisms account for 10 to 40% of all ischemic strokes. This range reflects varying definitions across series, evolution in diagnostic technology, differing conceptions of adequate etiologic investigation, and the fact that there are more than 200 known causes of ischemic stroke potentially requiring exclusion. In general, the percentage of ischemic strokes that are classified as cryptogenic has declined over time as diagnostic testing has advanced, from 40% in the 1970s to 10 to 15% today for highly cryptogenic stroke in advanced centers performing extensive testing. However, stroke that is cryptogenic after a standard diagnostic evaluation remains a common clinical challenge, accounting for 20 to 30% of all ischemic strokes and therefore occurring in 120,000 to 180,000 patients each year in the United States.
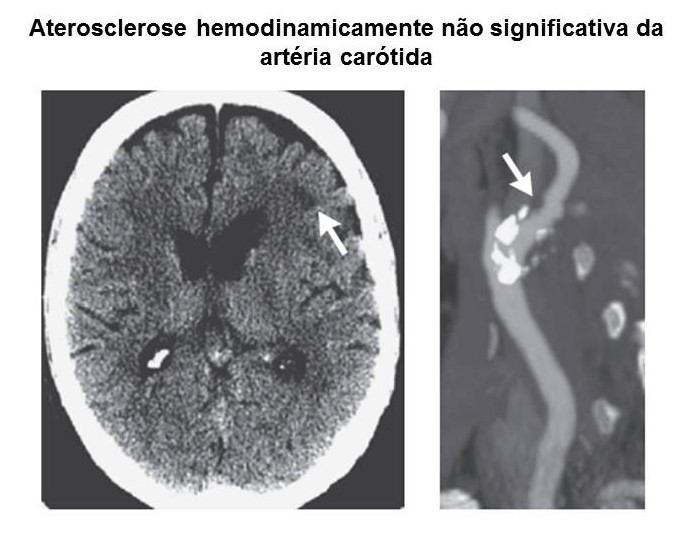
The most common determined causes of ischemic stroke, identified during routine initial evaluation, are large-artery atherosclerosis, cardioembolism, andsmall-vessel disease, each of which accounts for approximately 25% of cases. In patients with ischemic stroke that is considered to be cryptogenic after standard evaluation, causes that are most often found after more specialized testing include occult atherosclerosis, including nonstenosing but unstable plaques at intracranial and cervical sites or stenosing plaques at the thoracic origins of the common carotid and thoracic vertebral arteries; nonatherosclerotic arteriopathies, such as dissection or vasculitis; hypercoagulable states; cardioembolism from medium-grade sources, such as low-burden paroxysmal atrial fibrillation or dilated cardiomyopathy of moderate degree; and paradoxical embolism (Table S1 in the Supplementary Appendix, available with the full text of this article at NEJM.org).
The age of the patient influences the likelihood of various causes. In young adults 18 to 30 years of age, dissection is most common, but thrombophilias and congenital cardiac disease are also noteworthy causes. In persons 31 to 60 years of age, early-onset atherosclerosis and acquired structural cardiac disease are increasingly common. In patients older than 60 years of age, occult atrial fibrillation becomes more frequent.
As compared with strokes of determined origin, cryptogenic ischemic strokes typically result in less severe presenting neurologic deficits, less final disability, and lower mortality. In most though not all long-term follow-up studies, patients with cryptogenic ischemic stroke have a lower risk of recurrence than those with stroke of identified cause. In the largest long-term study to date, among patients 18 to 55 years ofage who had a stroke that was cryptogenic and who were treated with aspirin, the recurrence rate was 1.9% in the first year after the stroke and 0.8% per year in years 2 to 4. This low recurrence rate comports with the absence of an easily discovered cause of major stroke that would place the patient at elevated risk.
Fonte (Artigo na íntegra): http://www.nejm.org/